
People with PWS often struggle with puberty and sexual development and benefit from sex hormone therapy in their adolescent and adult years.
This is a result of hypogonadism – a condition where the body doesn’t produce enough sex hormones (testosterone for males, and estrogen and progesterone for females). These hormones are critical for preventing long-term complications, like osteoporosis, and support the natural progression through puberty.
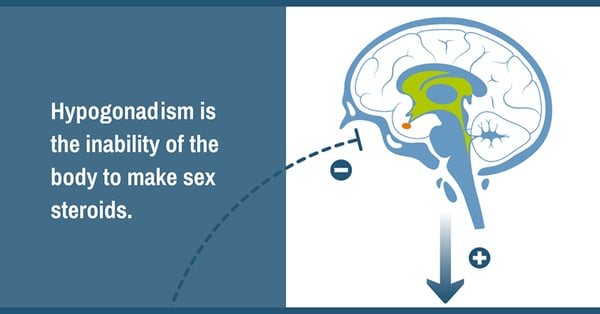
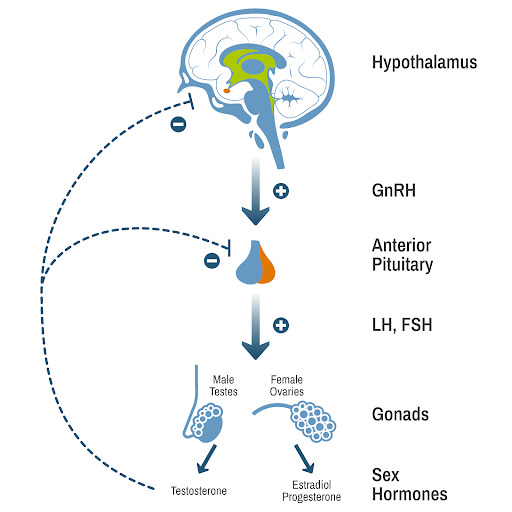
When a typically developing body reaches puberty, the brain starts to send out signals to the ovaries or testes to make estrogen or testosterone. When someone has hypogonadism, the signals are not sent, or the ovaries or testes are not able to respond to them.
The result is that the body does not produce the hormones needed for typical development.
There are two types of hypogonadism:
Hypogonadism is common in Prader-Willi syndrome (PWS), affecting at least half the people who have been diagnosed with the genetic disorder, and may be a combination of primary and/or secondary hypogonadism.
Our go-to expert on hypogonadism is Dr. Diane Stafford, pediatric endocrinologist and member of the PWS Clinical Investigation Collaborative, a group of clinical researchers, health care providers, and patient advocates working to improve care for people with PWS.
In a two-part video series for FPWR, Dr. Stafford provides an overview of the condition, addressing some of the most common questions about hypogonadism and sex steroid therapy.
Part 1 focuses on hypogonadism and the effect it has on the body. The second video covers more details on hypogonadism in the PWS population and explores treatment options.
The following symptoms are associated with hypogonadism:
In PWS, hypogonadism can present in several ways.
Scientists believe that hypogonadism in PWS is a result of the same hypothalamic dysfunction that causes growth hormone deficiency, hyperphagia, and other issues common in PWS.
However, they also speculate that the condition might be more complicated, as they are seeing some evidence of dysfunction involving the ovaries or testes as well.
Hypogonadism is a common symptom of PWS and affects both males and females. Hypogonadism is a life-long diagnosis, and it is likely that persons with PWS who need sex steroids at any point in their development/adulthood will need to continue to take them for the rest of their lives.



The Foundation for Prader-Willi Research (federal tax id 31-1763110) is a nonprofit corporation with federal tax exempt status as a public charity under section 501(c)(3).


![]()